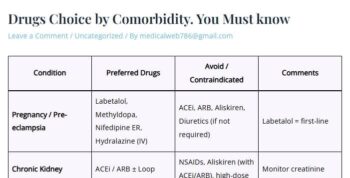
| Pregnancy / Pre-eclampsia | Labetalol, Methyldopa, Nifedipine ER, Hydralazine (IV) | ACEi, ARB, Aliskiren, Diuretics (if not required) | Labetalol = first-line |
| Chronic Kidney Disease (CKD) | ACEi / ARB ± Loop diuretic; Add CCB | NSAIDs, Aliskiren (with ACEi/ARB), high-dose K⁺ sparing | Monitor creatinine and potassium |
| Asthma / COPD | ARB, ACEi, CCB, Alpha-blocker | Non-selective beta-blockers | Bisoprolol/Nebivolol may be cautiously used |
| Chronic Liver Disease (CLD) | ACEi/ARB (low dose), Amlodipine | Methyldopa (hepatotoxicity), Minoxidil (fluid retention) | Dose titrate carefully |
| Heart Failure (HFrEF) | ACEi/ARB/ARNI + Beta-blocker (Bisoprolol, Carvedilol, Metoprolol) + MRA | Non-DHP CCB (Verapamil, Diltiazem) | Use loop diuretics for congestion |
| Diabetes Mellitus | ACEi/ARB + CCB or Thiazide | Beta-blockers (mask hypoglycemia) if no cardiac indication | Prefer ACEi/ARB to protect kidneys |
| Post-MI / CAD | Beta-blocker + ACEi/ARB | Dihydropyridine CCB (alone) | Add statin and antiplatelet as indicated |